Overview
Hello, HyGuru community! In this post, you’ll learn USMLE test taking strategies and integrations related to brain bleeds including:
- Epidural Hematomas
- Subdural hematomas
- Subarachnoid hemorrhages
Watch out for anatomy, pathophysiology, and pharmacology tie-ins and test yourself on the content at the end.. For more, check out our NBME Top Concepts Neurology video!
Brain Bleeds
- Epidural Hematoma
- Why is this also referred to as the ‘Talk & Die’ phenomenon?
- Because of its lucid interval
- Look for the following details in the vignette:
- Hit on the side of the head, bruising on the temple, or skull fracture
- Alert & oriented x 3 then dies 5 hours later
- A non-contrast CT showing, convex lens shape:

Item ID: 1499422511
- Anatomic Tie-in
- What is the affected artery?
- The middle meningeal off of the maxillary artery which branches off of the external carotid artery
- Through what foramen does the middle meningeal artery exit?
- The Foramen Spinosum
- What are 2 other major foramen and what exits through them?
- Rotundum→ maxillary division of trigeminal nerve
- Ovale→ Mandibular division of trigeminal nerve
- What is the affected artery?
- Subdural Hematoma
- Look for the following clinical scenarios
- Infant with bilateral retinal hemorrhages cause by shaking
- A nursing home resident who fell or an alcoholic
- Slow onset of symptoms
- Non contrast CT shows crescent-shaped lesion
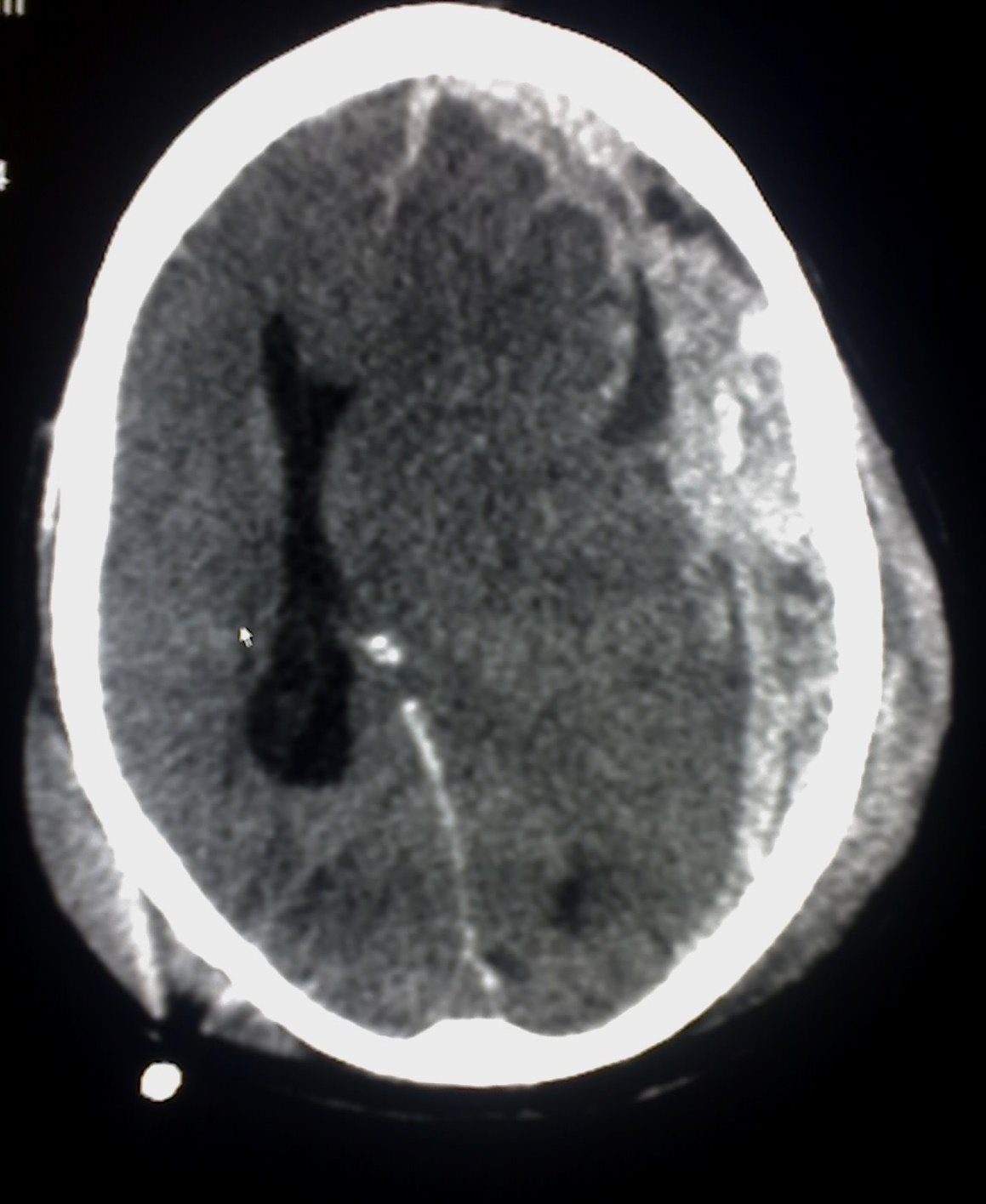
Item ID: 1730482000
- Pathophysiology Tie-In:
- How does bleeding occur?
- Atrophy of brain parenchyma leads to cellular shrinkage and bridge vein tearing
- How does bleeding occur?
- Subarachnoid Hemorrhage
- Quick question, what does thunderclap mean?
- Crash of thunder and it’s used to refer to something occurring suddenly or unexpectedly…much like the headache caused by a subarrachnoid
- Look for the following clinical clues
- Sudden onset headache with photophobia and vomiting
- History of polycystic kidney disease
- Xanthochromia of CSF (RBC breakdown)
- Non-contrast CT shows bleeding outlining sulci & gyri

- Anatomic Tie-In
- Where do Berry aneurysms ten to rupture and why?
- Junction of anterior cerebral and communicating arteries where the tunica media is weakest!
- What are the clinical and anatomic differences between Berry & Bouchard aneurysms?
- Berry→ sudden onset, thunderclap with a history of Marfans or ADPKD
- Bouchard→ gradual onset, thalamus or basal ganglia, history of long standing hypertension
- Where do Berry aneurysms ten to rupture and why?
- Bonus Pharmacology Tie-In
- Why is there in an increased risk of ischemic stroke after a subarrachnoid?
- Bleeding→ vasospasm→ ↑risk of ischemic stroke.
- What drug do you give to reduce this risk?
- Dihydropyridine (DHP) calcium channel blockers (CCB) e.g. nicardipine
- What are the non-DHP CCBs and where do they work?
- Diltiazem and verapamil work on the heart
- Why is there in an increased risk of ischemic stroke after a subarrachnoid?
Conclusion: Test Yourself
For each pathology, recreate the clinical scenario with its integrative tie-ins from memory!
- Epidural hematoma
- Clinical: Bruised temple, lucid interval, arterial bleed with convex lesion on CT
- Tie-In: From middle meningeal artery which exits through the foramen spinosum
- Subdural hematoma
- Clinical: Shaken baby, falling alcoholic or nursing home resident with slow symptom onset and crescent shaped lesion on CT
- Tie-In: parenchymal atrophy→ shearing of bridging veins
- Subarachnoid hemorrhage
- Clinical: Thunderclap sudden-onset headache with photophobia/vomiting in a Marfans or PCKD patient with CSF xanthochromia and bleeding tracing sulci and gyri on CT
- Tie-In: from berry aneurysm rupture at anterior cerebral and communicating arterial junction (weak tunica media). Prevent ischemic stroke complications with DHP CCBs.
Like this post? For more, check out our NBME Top Concepts Neurology video! Or link to our other neurology posts here.